Syringes-pens with insulin, which we use daily, can be stored at room temperature.
Insulin overheating is also not allowed. In summer we should not be exposed to direct sunlight.
We must have insulin in our handbag when traveling by plane. Do not carry insulin in your luggage.
When storage rules are not followed, insulin may leak and change color.
Insulin concentration
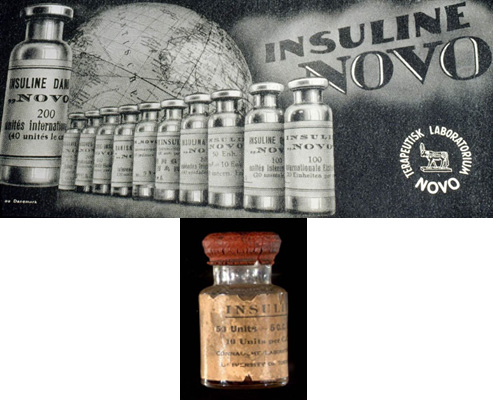
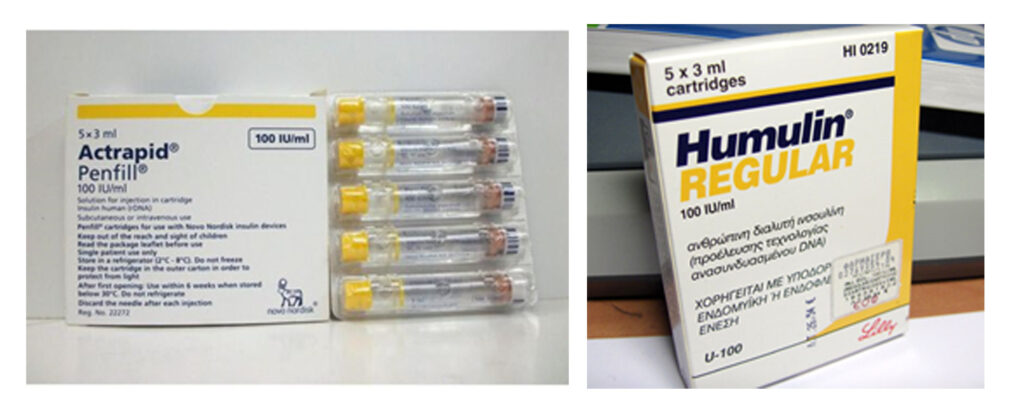
Today, insulin is mainly used all over the world, with a concentration of 100 units per ml.
In the past we found insulin with a concentration of 40 units per ml. Each cartridge is labeled with a concentration label.
Older, 40-unit syringes for insulin can still be found in pharmacies. Therefore, when using syringes, we must buy special 100-unit syringes so as not to confuse the doses.
Factors that affect the action of insulin:
While we may get identical doses of insulin over several days and the food may be exactly the same, it is quite possible to get different glycemic indexes.
There are many factors that affect the action of insulin, including:
Subcutaneous blood supply: increases with heating: eg sauna, jacuzzi, shower, bath, high temperature. Decreases: as a result of colds, tobacco consumption, dehydration.
Injection depth. It is absorbed faster from the muscle.
Injection site. It is absorbed most quickly from the abdomen, most slowly from the thigh.
Antibodies to insulin. Binds to insulin and lowers its action
Physical activity. Insulin is absorbed faster.
Massage the injection site. It is also absorbed faster.
Thickness of subcutaneous adipose tissue. The thicker it is, the slower it is absorbed
Injection in lipodystrophies.- Absorbed more slowly
What happens if a child refuses to eat?
In such a case, if the child is taking ultra-short-acting insulin, we do it after the meal, in reduced quantities, according to the food taken.
And if the child is on short-term insulin and we have already given the appropriate injection, then somehow we have to fill the acceptable bread units, we can offer more bread, which is usually less refused.
You may find yourself in a situation where you miss an insulin injection, what should we do?
It depends on which dose is missed:
1, dose before meals. If you remember soon, do the same dose as soon as you remember, or 1-2 units less, if 1-2 hours have elapsed, do half the dose, and if even more, add the next dose according to your glycemic index.
2, pre-sleep dose: If we are taking prolonged-acting insulin and remember it before 2pm, we are doing a 25-30% lower dose, or 1-2 units less, with each passing hour. If less than 5 hours remain before the morning injection, inject a half-dose of short-acting insulin, or 0.1 one / kg body weight.
If we take long-acting insulin, we do the usual dose in case of rapid recall, if we remember in the morning and we usually take insulin once a day, we do half the dose, or twice, we do the morning dose and we correct the glycemia with ultra-short insulin.